You’re Taking Your Stimulants at the Wrong Time
Dopamine runs on a four-hour clock that you didn’t know about.
If you have ADHD, you might have noticed that sometimes your stimulants work, and sometimes they don’t do much. You ask your doctor about it, the usual reply is that it’s related to sleep or hormonal changes or something else of the sort. Then you track it and can’t find any obvious pattern.
I often take stimulants, and I usually take them at random times throughout the day. What I noticed is that sometimes taking a stimulant would produce almost no effect, whereas some other time taking the same dose would produce a very strong stimulatory effect, almost uncomfortable. And on other days it would just be a normal response, without any particularities. This couldn’t be tied to a circadian clock. What else could it be?
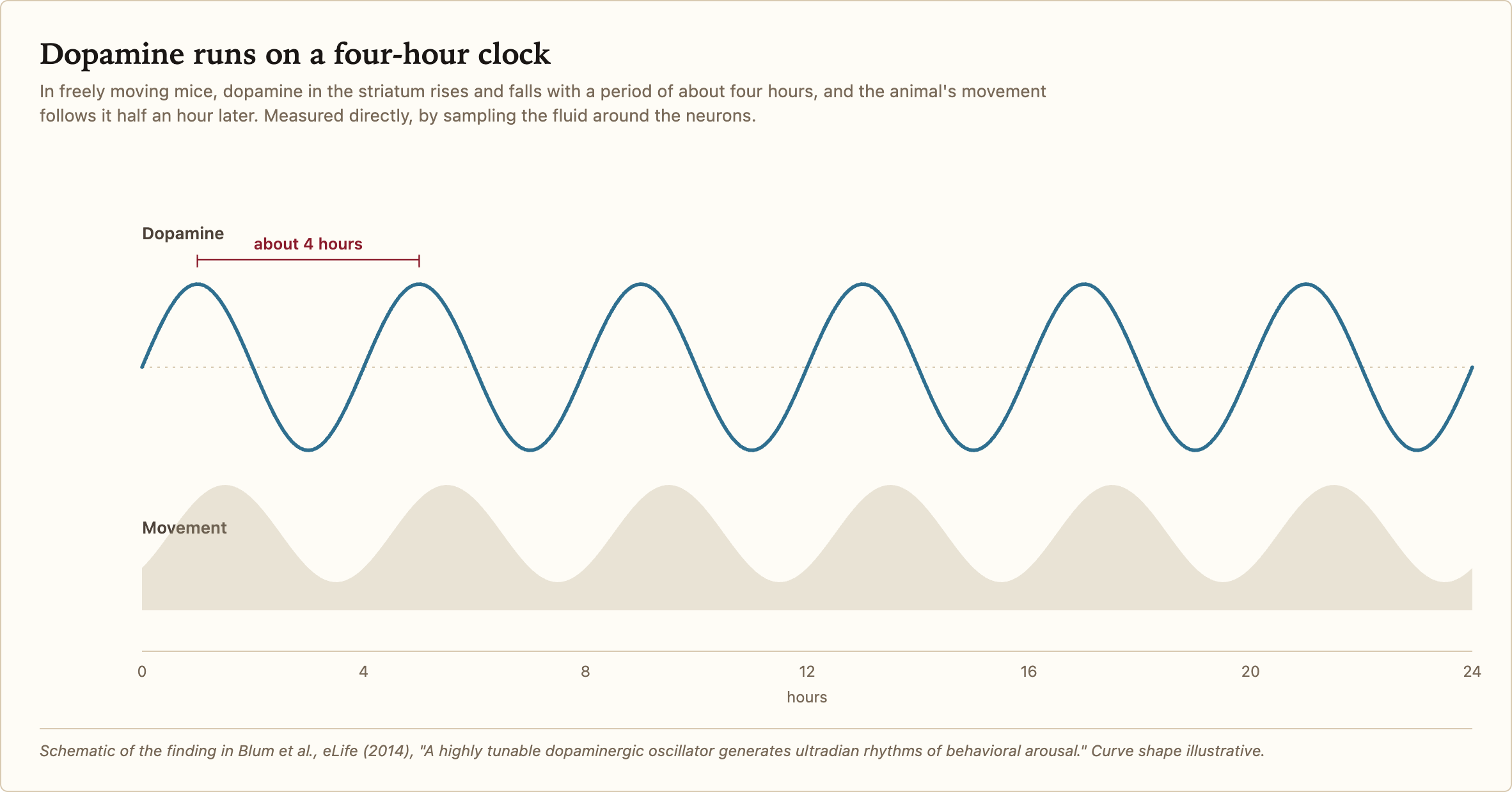
In 2014, scientists implanted a microdialysis probe into a mouse brain to determine the levels of dopamine. What they found was that the levels oscillated with a periodicity of four hours. When the levels were high the mouse would run around in its cage and when the levels were low the mouse would rest. They termed it the Dopamine Ultradian Oscillator (DUO).
You’d think it’s related to the circadian rhythm, but even when mice had the suprachiasmatic nucleus (the body’s circadian clock) surgically lesioned, their DUO was intact. It’s an independent cycle.
I have a non-24-hour sleep-wake disorder, so my days are about 32 hours long. This makes it complicated to properly judge circadian rhythm issues, because generally your circadian clock is entrained by light, which obviously isn’t the case for me. But what about my dopamine ultradian cycle?
This cycle has only ever been measured directly in mice, but behavioural rhythms consistent with it do show up in people. And a mathematical model was built to try to explain the different effects you can get from stimulants depending on when and how you’re taking them.
I’m a human version of the SCN-lesioned mouse: my circadian clock free-runs against the calendar instead of locking to it. And I still can’t predict which response I’ll get from a given dose, which is exactly what you’d expect if the response comes not from the circadian rhythm, but from something faster underneath.
The scientists tried adding methamphetamine to the mice’s drinking water, to see whether it would affect the cycles. And it did, the cycles went from ~4 hours to up to ~48 hours, depending on the dose. This means this clock is tuned by dopamine manipulation. We don’t exactly know how it behaves in humans, but it’s reasonable to assume that, given mice are also mammals and share much of their neuroanatomy with us, we also have these clocks, and that we also likely have them extended when we use stimulants. That would explain a lot of the effects.
In 2025, another group confirmed the same thing in a different strain of mice: chronic methamphetamine stretched the ultradian cycle and, on top of that, spawned a new ~48-hour band. The authors say this “may explain the sleep-wake disturbances reported in individuals treated with stimulants, especially those with ADHD.”
So, you have the circadian rhythm that’s normally 24 hours in humans. Normally, when you wake up in the morning, this induces a rise in cortisol, which in turn wakes your system up. Then, throughout the day, adenosine accumulates, the same adenosine that’s blocked by coffee, by the way. And as the day progresses and gets closer to evening, the body starts producing melatonin. Together with adenosine, that creates the sleepy feeling that prepares the body for sleep.
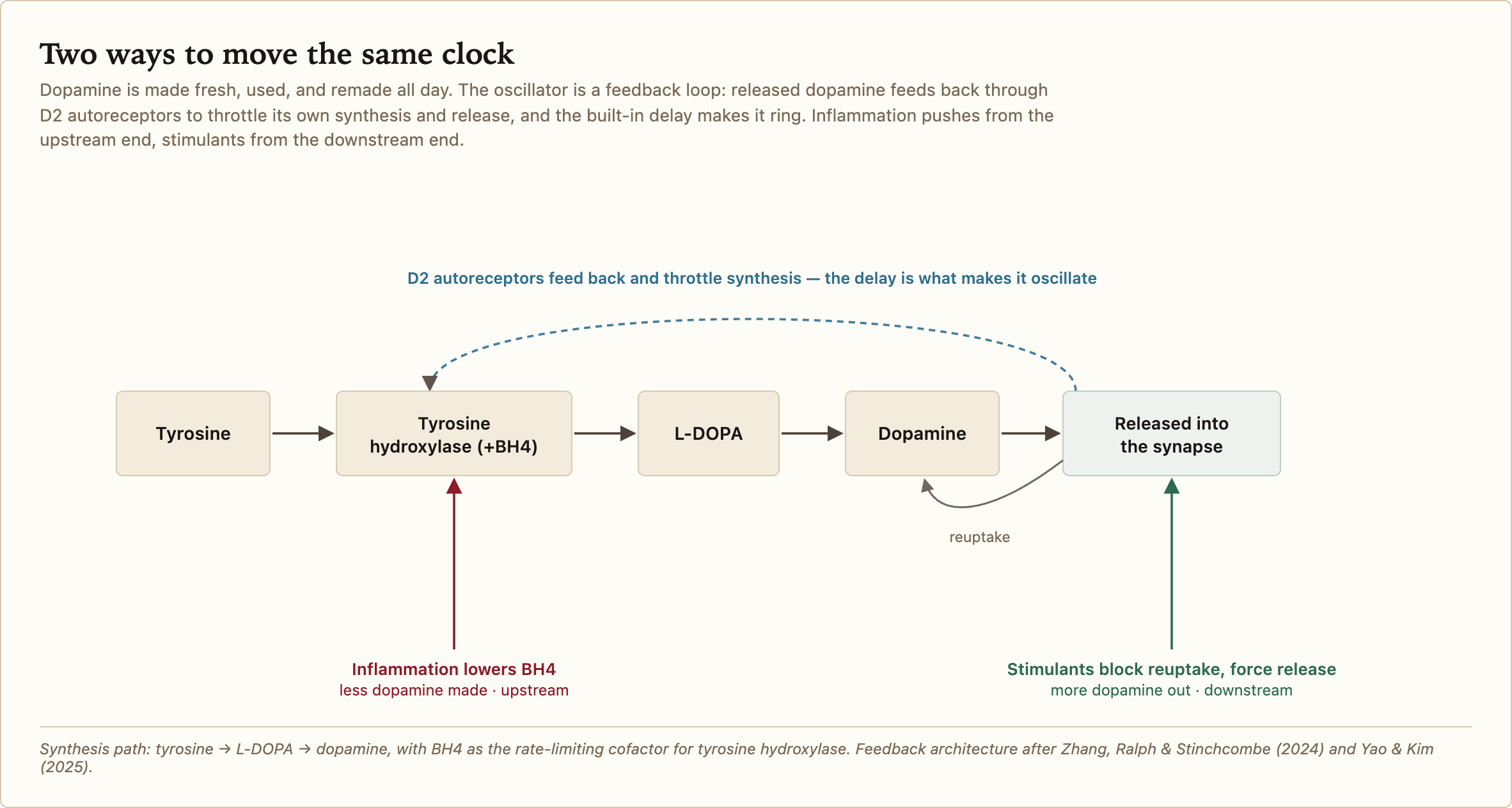
And on top of that, you also have the dopamine ultradian cycle that’s normally 4 hours, but this can vary with stimulants. The cycle itself, though, isn’t created by them. It’s present even in mice that have never seen a stimulant. The engine is a feedback loop: dopamine sitting in the extracellular space activates D2 autoreceptors on the dopamine terminals, and those autoreceptors throttle further release and ramp up reuptake. Because synthesis and reuptake both take time, the loop has a built-in delay, and a negative feedback loop with a delay is the textbook recipe for an oscillation. What a stimulant does is push on this loop from the outside and stretch its period. Interestingly, going past ~26% reuptake inhibition just flatlines the oscillation completely.
Another clock that has been shown in humans in more detail is the 90-minute basic rest-activity cycle, or BRAC. This one is identified as the REM cycle from sleep persisting into waking. Note that the DUO is not the BRAC.
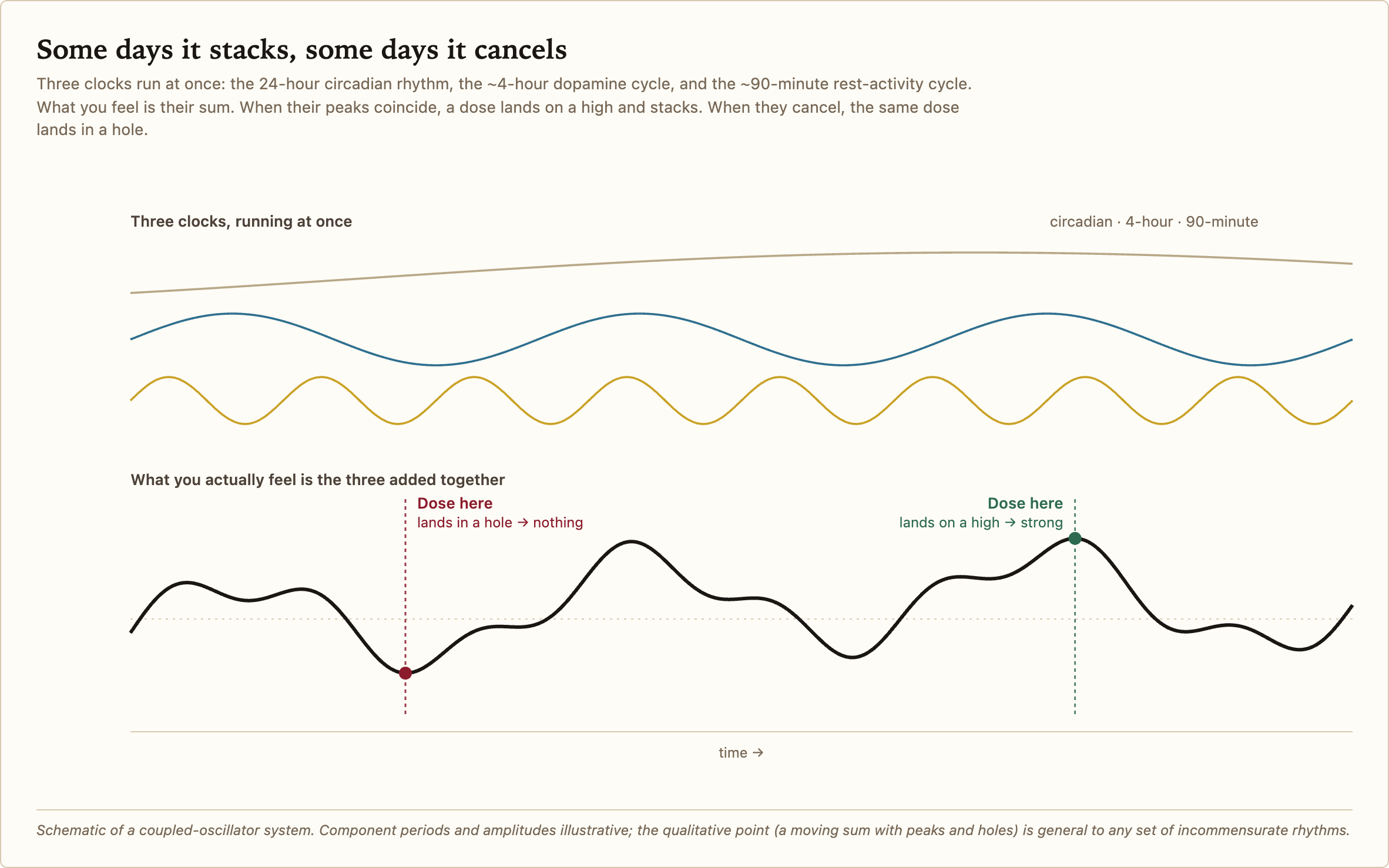
As you may remember from physics, waves can interfere additively or destructively. Normally those cycles are entrained to each other, which means their peaks and troughs are lined up in such a way that you naturally get a boost of energy during the day and restful sleep at night.
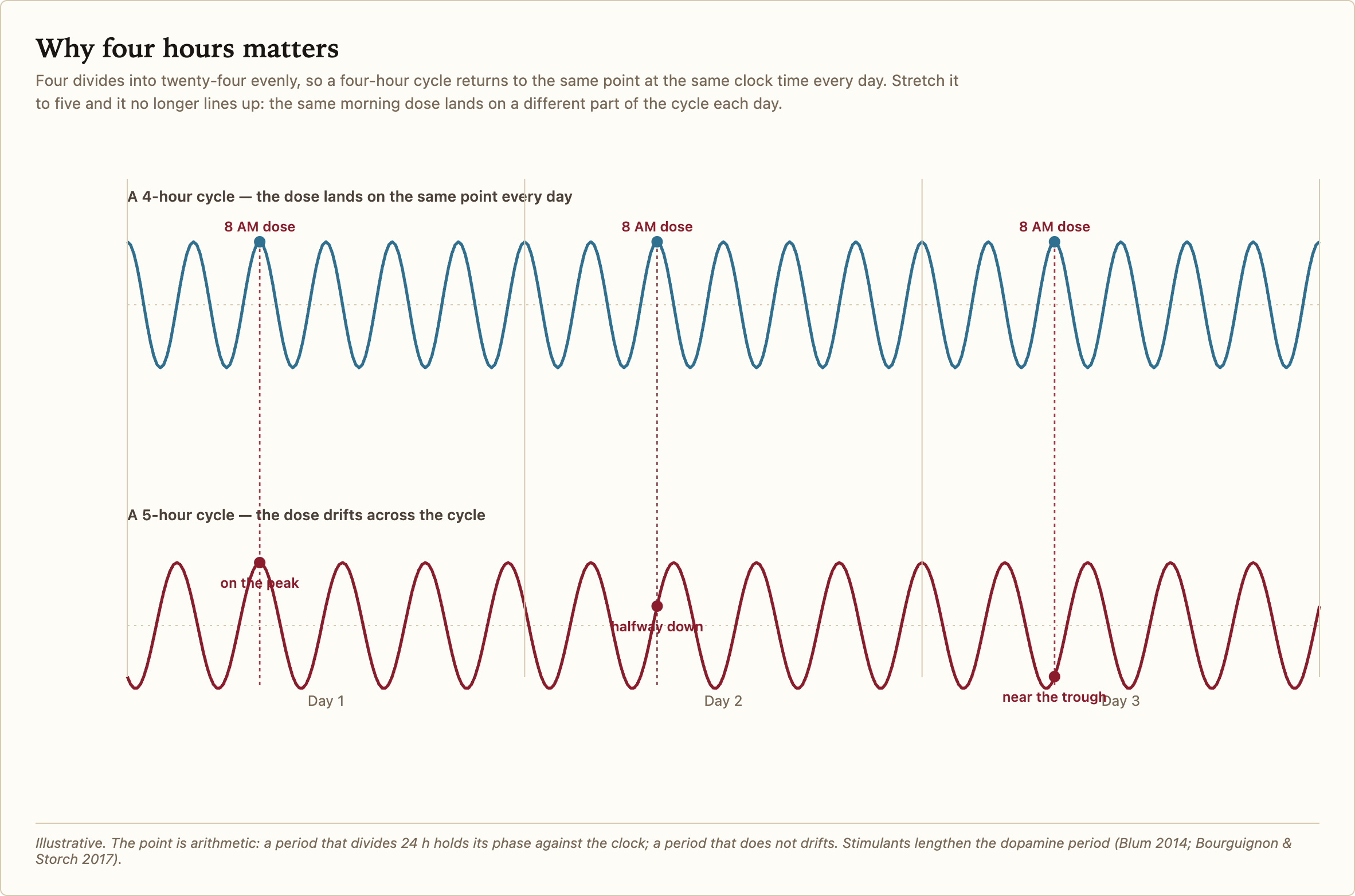
But we just learned that taking stimulants can extend the period of the DUO way past four hours. Four hours is important. 24 ÷ 4 = 6, that’s a whole number, so the cycle comes back to the same phase at the same clock time every day. But what if it gets extended to, say, five hours? 24 ÷ 5 = 4.8, which won’t align with your circadian rhythm at all. At the same time every day, you’ll be at a different phase.
Now, a little bit about dopamine. The dopamine system has two distinct modes: tonic and phasic dopamine.
When you tap a button on a slot machine and you win, this is a positive signal. It feels good. What the dopamine encodes is called a prediction error, whether the outcome is better or worse than expected. When you don’t win, there is no prediction error at all, because the brain already predicts that you won’t win, so there is nothing to learn. Now suppose there’s an additional slot on the slot machine that, when hit, electrocutes you. If you land on that, you get a negative prediction error. That feels bad! Those events teach you something about the world, and are called phasic.
What about the general mood, the sense of what kind of rewards you can expect? This is encoded by what’s called tonic dopamine, which is just the baseline level of activation of dopamine neurons. When you’re in an environment where a lot of positive rewards can be expected, your tonic dopamine rises. And once you approach something desirable, your tonic dopamine also rises, in anticipation of a future reward. If instead you keep doing things that result in no rewards, or in negative ones, then your tonic levels eventually drop.
Normally, in people without ADHD, the tonic level never drops low enough that they can’t focus or initiate new activities. But that’s not the case with ADHD. With ADHD, your dopamine levels can drop to a point where you can’t initiate actions even when you want to.
So what about the dopamine rhythms? To put it simply, they are tonic dopamine fluctuations, not phasic. This means that when you’re in the up portion of the cycle, your body assumes you’re in an environment where rewards are more likely, so it makes more sense to expend energy. And when you’re in a trough, it means rewards are unlikely, and you’re better off conserving energy by doing nothing, or doing cheap, easy tasks.
And here we get to the stimulants. Normally the purpose of a stimulant is to raise your dopamine levels, because higher dopamine increases your willingness to approach and interact with the world.
You shouldn’t assume it’s just the dopamine that matters. What also matters is the sensitivity of your neurons to dopamine. If your neurons are insensitive, then no matter how much dopamine is there, the neurons just don’t care. This is what explains, for example, the rapid tachyphylaxis of amphetamines. Amphetamine has a very long half-life, around 10 hours, but its action does not last for ten hours. This is mostly a presynaptic effect: amphetamine releases so much dopamine that the readily-releasable pool gets drained faster than it can be refilled, and the receptors desensitize on top of that, so the neuron simply runs out of dopamine to release.
What happens when you take a stimulant while you’re at the low point of your dopamine cycle? Not much. You don’t have enough activity; you take a stimulant and it raises that activity, but only a little, because stimulants don’t simply make the neurons fire. They work by increasing dopamine concentrations, either by blocking what’s called the reuptake of dopamine or by releasing dopamine into the synaptic cleft. If you don’t have enough dopamine, or if your neurons aren’t sensitive enough to it, then it doesn’t really matter what the stimulant does. You’re still not going to do much.
Your neurons also need to have enough dopamine to be able to release it. Contrary to what you might think, dopamine is constantly recycled. It is constantly being synthesized, used, destroyed, and then synthesized again. Dopamine molecules don’t sit there all day. The body produces dopamine from tyrosine, which is commonly found in food. To make it, it needs an enzyme that’s called tyrosine hydroxylase. Together with a cofactor called BH4, it converts tyrosine into levodopa. And levodopa is then converted to dopamine. Disruptions to any of them can lead to your body not having enough dopamine.
What can cause disruptions? Chronic inflammation, for example. That one significantly reduces the BH4 cofactor availability. BH4 is the rate-limiting factor for tyrosine hydroxylase: without it, the enzyme won’t convert anything. And chronic inflammation is something that is quite commonly comorbid with ADHD.
Some hepatitis C patients are treated with a drug called interferon-alpha. It drives up inflammation to help fight the virus. What it also does is make a lot of the patients slide into depression. Some of them were put in a PET scanner to see what was happening. The dopamine precursor still went into the striatum, but much less dopamine came back out, and the less dopamine came out the more depressed they felt. But when dopamine output is suppressed this way, giving levodopa, the raw material one step downstream, restores it.
So there are at least two ways to retune the same oscillator. Stimulants push on it from the downstream side, and inflammation starves it from the upstream side, and that second route reaches well beyond ADHD, into ordinary depression. This complicates the textbook story. The conventional picture of ADHD is simple: too little dopamine signaling, corrected by a stimulant. The advice that follows is just as simple: take the stimulant every day at the same time, usually in the morning. But if the thing you’re dosing is a moving oscillator with more than one input, a fixed morning dose might not work as reliably as you’d think.
We know from testing that certain drugs work best when taken at specific points in time. For example, modafinil works best when given during the circadian trough, which is at night. Parkinson’s patients take levodopa as a medication, and the same daily levodopa dose, depending on whether it’s delivered pulsatile or smooth (infusion pump), can give you dyskinesia or not. And we also know that bupropion, a popular stimulant and antidepressant, has different effects in people with different circadian genes. Medicine has been taking timing seriously for a long time, just not for stimulants.
So what we have, in the end, is three clocks. One is the SCN circadian clock, at 24 hours. One is the dopamine ultradian oscillator, 4 hours at baseline, but it can be retuned to 8, up to 48 hours, by stimulants. And then you have the BRAC, which is normally 90 minutes.
Stimulants move the DUO; the other two don’t need to move. But if you look at their interference pattern, you’ll notice something interesting. Days where the dose lands at constructive interference are the days it synergizes, whereas days where it lands at destructive interference are the days it does nothing. The corollary is that same-clock-time dosing is a bad strategy, because, as we found, the clock might move, so taking the dose at a fixed time, when you might be in the trough, can just waste the stimulant.
In a mouse you can sample the dopamine in the synaptic cleft directly with a probe, but you can’t put one into a living human striatum. So on the human side we’re inferring the cycle from behaviour and from PET imaging, rather than measuring it directly. When I take a stimulant and feel nothing, I am most likely in the trough. When it’s almost too much I am at the constructive peak, and when it’s normal I’m somewhere in between. I’m now trying to take stimulants only when I’m on the rising phase, although it’s hard with my cycles. Next time try to find the same oscillation in yourself, and maybe try taking the stimulant at the rising phase.
References
Blum ID, Zhu L, Moquin L, et al. A highly tunable dopaminergic oscillator generates ultradian rhythms of behavioral arousal. eLife 3:e05105 (2014). doi:10.7554/eLife.05105
Bourguignon C, Storch KF. Control of rest:activity by a dopaminergic ultradian oscillator and the circadian clock. Frontiers in Neurology 8:614 (2017). doi:10.3389/fneur.2017.00614
Barnes SA, Alanazi N, Yamazaki S, Stefanovska A. Methamphetamine alters the circadian oscillator and its couplings on multiple scales in Per1/2/3 knockout mice. PNAS Nexus (2025). doi:10.1093/pnasnexus/pgaf070
Zhang AQ, Ralph MR, Stinchcombe AR. A mathematical model for the role of dopamine-D2 self-regulation in the production of ultradian rhythms. PLOS Computational Biology 20(5):e1012082 (2024). doi:10.1371/journal.pcbi.1012082
Yao T, Kim R. Mathematical modeling of dopamine rhythms and timing of dopamine reuptake inhibitors. PLOS Computational Biology 21(9):e1013508 (2025). doi:10.1371/journal.pcbi.1013508
Grace AA. Phasic versus tonic dopamine release and the modulation of dopamine system responsivity: a hypothesis for the etiology of schizophrenia. Neuroscience 41(1):1–24 (1991). doi:10.1016/0306-4522(91)90196-U
Kripke DF. An ultradian biologic rhythm associated with perceptual deprivation and REM sleep. Psychosomatic Medicine 34(3):221–34 (1972). doi:10.1097/00006842-197205000-00005
Capuron L, Pagnoni G, Drake DF, et al. Dopaminergic mechanisms of reduced basal ganglia responses to hedonic reward during interferon alfa administration. Archives of General Psychiatry 69(10):1044–53 (2012). doi:10.1001/archgenpsychiatry.2011.2094
Felger JC, Hernandez CR, Miller AH. Levodopa reverses cytokine-induced reductions in striatal dopamine release. International Journal of Neuropsychopharmacology 18(4):pyu084 (2015). doi:10.1093/ijnp/pyu084
Wesensten NJ, Belenky G, Kautz MA, et al. Maintaining alertness and performance during sleep deprivation: modafinil versus caffeine. Psychopharmacology 159(3):238–47 (2002). doi:10.1007/s002130100916
Olanow CW, Obeso JA, Stocchi F. Continuous dopamine-receptor treatment of Parkinson’s disease: scientific rationale and clinical implications. Lancet Neurology 5(8):677–87 (2006). doi:10.1016/S1474-4422(06)70521-X
Li QS, Tian C, et al. Analysis of 23andMe antidepressant efficacy survey data: implication of circadian rhythm and neuroplasticity in bupropion response. Translational Psychiatry 6:e889 (2016). doi:10.1038/tp.2016.171
Entered this 29th day of May, by ✚ 陽炎 ✚